
Share on twittShare on linkediShare on faceboShare on emaiShare

Image: mapasa/iStock
Some 5 to 17 percent of all children have developmental dyslexia, or unexplained reading difficulty. When a parent has dyslexia, the odds jump to 50 percent.
Typically, though, dyslexia isn’t diagnosed until the end of second grade or as late as third grade, when interventions are less effective and self-esteem has already suffered.
“It’s a diagnosis that requires failure,” said Nadine Gaab, Harvard Medical School associate professor of pediatrics in the Laboratories of Cognitive Neuroscience at Boston Children’s Hospital.
A new study in the journal Cerebral Cortex led by Gaab and lab members Nicolas Langer and Barbara Peysakhovich has found that the writing is on the wall as early as infancy—if only there were a way to read it and intervene before the academic, social and emotional damage is done.
In 2012, the Gaab Lab showed that pre-readers with a family history of dyslexia (average age 5½) have differences in the left hemisphere of their brains, according to magnetic resonance imaging (MRI).
“The first day they step in a kindergarten classroom, they are already less well-equipped to learn to read,” Gaab said.
Some researchers have proposed that the difference reflects being raised by a dyslexic parent—perhaps, for example, being read to less. But could the difference be innate?
To answer this question, Gaab and colleagues performed advanced MRI brain imaging on 14 infants with a family history of dyslexia and 18 infants of similar age with no such family history.
Since infants need to be completely still inside the scanner, this required an elaborate protocol, developed with the help of Ellen Grant, HMS associate professor of radiology and director of the Fetal-Neonatal Neuroimaging and Developmental Science Center at Boston Children’s.
Parents brought their babies in for scanning before their best naptime, early enough that they wouldn’t fall asleep in the car, and settled them in a space that was intended to mimic the babies’ home sleep environment. Time was built in to allow babies to get used to the sound of the MRI machine.
Once parents got their babies off to sleep, Gaab’s team carefully slid the infants into the scanner. This strategy worked about 70 percent of the time.
The MRI scan included an advanced technique called diffusion tensor imaging (DTI). It measures the flow of water molecules along the brain’s fiber tracts, and gives a good indication of how the fibers are structured and oriented and how well information is flowing in the brain.
As reported in the new study, the scan found alterations in a particular structure called the arcuate fasciculus, a bundle of fibers that connects the posterior cortex, which is involved in mapping sounds and word/letter recognition, with the frontal cortex, which integrates and comprehends this information.
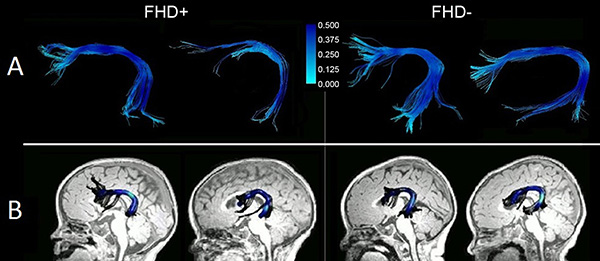 The arcuate fasciculus in a child with a family history of dyslexia (L) versus no family history (R), as seen on DTI. Image: Nicolas Langer and Barbara PeysakhovichDetailed segmentation of the images revealed that fibers in certain areas of the arcuate fasciculus were consistently less organized.
The arcuate fasciculus in a child with a family history of dyslexia (L) versus no family history (R), as seen on DTI. Image: Nicolas Langer and Barbara PeysakhovichDetailed segmentation of the images revealed that fibers in certain areas of the arcuate fasciculus were consistently less organized.
People who have suffered damage to the arcuate fasciculus are known to have problems with expressive and receptive language and with phonological processing—the ability to manipulate the sounds of a language, a critical part of learning to read. In infants with familial dyslexia, inherited genes may interfere with the prenatal development of the arcuate fasciculus, said Gaab, impairing its structural integrity.
“The street could be full of potholes, or it could be the street is narrow or has a really crappy surface, or there might be a lot of intersections where you have to stop,” she said.
But biology isn’t necessarily destiny. Research shows that with early interventions, 50 to 90 percent of children with dyslexia can become good readers, said Gaab. There are even studies indicating that the interventions lead to normalization of white matter pathways in the brain’s left hemisphere.
But while public health studies support early intervention for dyslexia, many schools shy away from screening, lacking the resources to test and intervene.
“We hope this study will help show that kids should get interventions before kindergarten,” said Gaab. “We’re not saying you should scan every kindergartner, but if you have a strong family history, you could potentially have a five-minute DTI scan to see if you are at risk.”
Adapted from a post on Vector, the clinical and research innovation blog at Boston Children’s.
Source hms.harvard.edu




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}